Acute exacerbation of bronchial asthma with type 2 diabetes mellitus
This is an online E logbook to discuss our patients' de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through a series of inputs from the available global online community of experts intending to solve those patients' clinical problems with the collective current best evidence-based inputs.
This e-log book also reflects my patient-centered online learning portfolio and your valuable inputs.
I have been given this case to solve in an attempt to understand the topic of " Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, and investigations, and come up with a diagnosis and treatment plan.
This is a case of 70 year old female resident of miryalaguda came with the
Chief Complaints:
Shortness of breath since 2 months
HOPI:
The patient was apparently asymptomatic 2 months back then she developed shortness of breath which was insidious in onset and gradually progessive associated with wheeze when exposed to cold and dust aggrevated on lying down in bed and relieved on sitting
Patient also had a complaint of dry cough occasionally which last for 1 week and with no aggrevating and relieving factors.
No h/o of fever, chest pain ,chest tightness,hemoptysis, sweating and palpitations .
Past history:-
K/c/o asthma , diabetes mellitus -2,
No history of tb, htn , epilepsy, thyroid disorders.
Family History: elder sister- k/c/o Asthma since childhood
Personal history:-
Diet:- mixed
Appetite :-normal
Bowel and bladder :- regular and normal
Addictions:- none
Treatment history:- patient was using Rota haler (fluticasone) , medication for diabetes.
General examination: -
The patient is conscious, coherent, cooperative and well oriented to time place and person.
Vitals:-
Pulse rate : 110beats /mim
Rr: 20 cpm
Bp: 130/80mmhg.
Temp: afebrile
Spo2:96
No pallor
No icterus
No cyanosis
No clubbing
No palpable lymphnodes
Edema:- bilateral pitting type of edema upto ankles


Systemic examination:
Rs:
Inspection:
Shape of the chest -Barrel shaped
Trachea position is central
Symmetrical movements of the chest with
respiration.
No presence of any sinuses , scars, engorged veins
Palpation:
No rise if temperature and no tenderness
All inspiratory findings are confirmed
Percussion:
Resonant note is Heard
Ascultation:
Vesicular breath sounds heard
Bilateral basal crepitations and wheese are heard.
CVS:
S1 s2 heard with no murmers
CNS: all higher mental functions,cranial nerves,motorsystem and sensory system are intact.
Normal speech observed.
Perabdomen:
Abdomen is obese
No palpable spleen ,liver, lymphnodes.

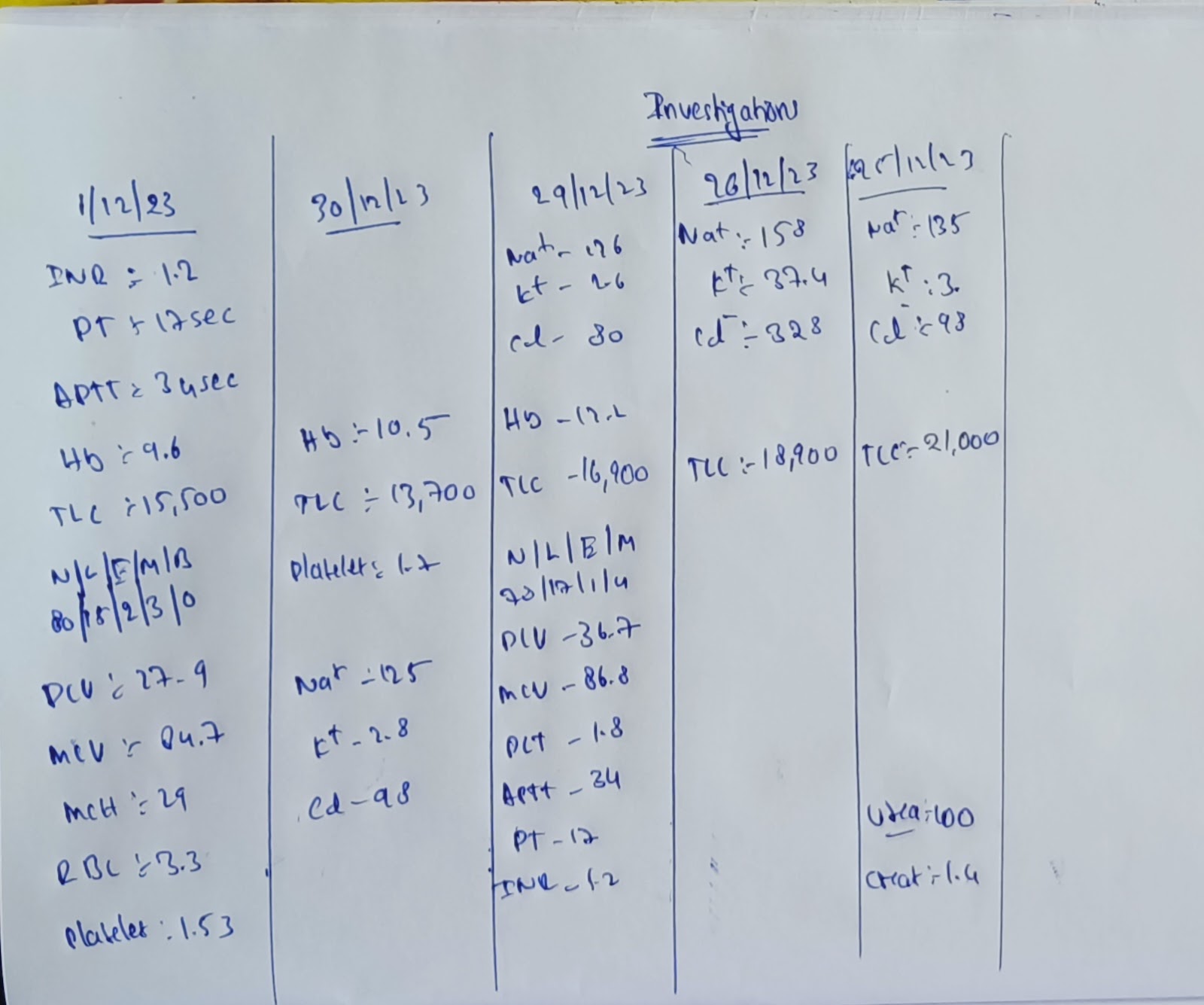
Investigations:-


Provisional Diagnosis:-
Acute exacerbation of asthma with diabetes mellitus type 2
Treatment:-
Budesonide nebulizer suspension
Inj augmentin iv /tid
Inj pan 40mg iv/od
Inj lasix 40mg iv/bd
Inj hydrocortisone 100mg iv/bd
Insulin subcutaneous/tid
Inj noh s/c bd
Tab azithromycin
Tab prednisolone


Comments
Post a Comment